

The labrum is a pad between the ball and socket joint of the shoulder. There are two general types of labral tears. One is from a fall or other traumatic event, while the other type usually occurs from repetitive overload. Read on to learn more about shoulder labral tears and which types tend to need surgery and what group of athletes and labral tears may actually do worse after surgical repair.
A BRIEF DISCUSSION OF SHOULDER ANATOMY
The shoulder is actually not one joint, but three different joints:
 The connection between the collarbone (clavicle) and the shoulder girdle (scapula) is known as the acromioclavicular or “AC Joint.”
The connection between the collarbone (clavicle) and the shoulder girdle (scapula) is known as the acromioclavicular or “AC Joint.”- The connection between the shoulder girdle (scapula) and the rib cage is known as the scapulothoracic joint.
- The “ball and socket” joint between humeral head (ball) and glenoid portion (socket) of the shoulder girdle is also known as the glenohumeral joint. This is what most people think of when speaking about shoulder joints.
 The connection between the collarbone (clavicle) and the shoulder girdle (scapula) is known as the acromioclavicular or “AC Joint.”
The connection between the collarbone (clavicle) and the shoulder girdle (scapula) is known as the acromioclavicular or “AC Joint.”Limitations in movement of each of these joints can impact the health of the shoulder labrum, especially in the case of repetitive overload injuries (stay tuned for more details below).
 The labrum (located between the ball and socket joint of the shoulder) is a fibrocartilage pad attached to the glenoid and provides stability of the glenohumeral joint by limiting excessive forward, backward, and downward movement of the humerus. The rotator cuff muscles that are in front, above and behind the glenohumeral joint also help to provide more stability.
The labrum (located between the ball and socket joint of the shoulder) is a fibrocartilage pad attached to the glenoid and provides stability of the glenohumeral joint by limiting excessive forward, backward, and downward movement of the humerus. The rotator cuff muscles that are in front, above and behind the glenohumeral joint also help to provide more stability.
TYPES AND CAUSES OF SHOULDER LABRAL TEARS
ACUTE TRAUMATIC SHOULDER LABRAL TEAR
Acute traumatic shoulder labral tears often occur when the arm is used to protect or support the body during a fall. Another common traumatic labral tear comes from having the upper arm and elbow pulled backward causing excessive forward motion of the humeral head.
The ball of the arm might come partially (called a glenohumeral subluxation) or completely (called a glenohumeral dislocation) out of the socket. A subluxation usually quickly goes back into normal position. Most dislocations are anterior (ball ends up in front of the socket) and require manipulation and medication to be able to put the arm back into its normal position.
Labral tears are commonly seen after dislocations (somewhat less often with subluxations). The most frequent tear after an anterior dislocation is in the anterior and inferior part of the labrum and glenohumeral joint capsule. This is called a Bankart lesion and may pull off part of the glenoid bone (boney Bankart).
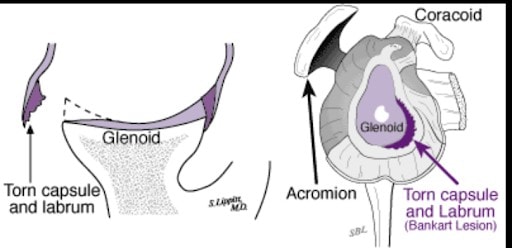
Picture of Bankart lesion courtesy of:
 These acute traumatic labral tears have a high risk for future glenohumeral joint instability episodes such as subluxation and dislocations of the shoulder. Some patients report a sense of abnormal movement and instability in the shoulder especially when in the “danger position” shown below.
These acute traumatic labral tears have a high risk for future glenohumeral joint instability episodes such as subluxation and dislocations of the shoulder. Some patients report a sense of abnormal movement and instability in the shoulder especially when in the “danger position” shown below.
Due to the high chance of re-injury and instability, tears in the front and lower part of the shoulder labrum more frequently require surgical repair. This includes fixing the labrum and often tightening the capsule surrounding the glenohumeral joint. Any damage to the rotator cuff muscles can also be repaired if needed. Surgical repair does not fully eliminate risk of future instability, but it does reduce the chances of future episodes.
REPETITIVE OVERLOAD SHOULDER LABRAL TEARS
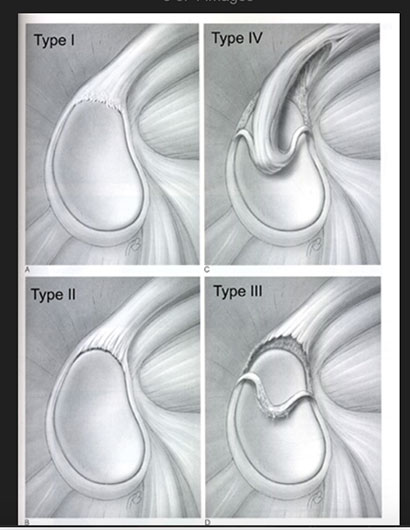 Overhead motions such as throwing/pitching a baseball, hitting a volleyball, or serving a tennis ball put repetitive stresses on the labrum and glenohumeral joint. The area of most common repetitive overload injury is at the top (superior) aspect of the labrum, and the injury may be in both the front and back part of this superior labrum. This is where one of the two tendons from the biceps brachii muscle (long head) attaches to the labrum and rim of the glenoid bone. A common name for this type of tears is a SLAP lesion which stands for Superior Labrum Anterior to Posterior.
Overhead motions such as throwing/pitching a baseball, hitting a volleyball, or serving a tennis ball put repetitive stresses on the labrum and glenohumeral joint. The area of most common repetitive overload injury is at the top (superior) aspect of the labrum, and the injury may be in both the front and back part of this superior labrum. This is where one of the two tendons from the biceps brachii muscle (long head) attaches to the labrum and rim of the glenoid bone. A common name for this type of tears is a SLAP lesion which stands for Superior Labrum Anterior to Posterior.
Figure: Types of SLAP tears courtesy of https://www.orthobullets.com/shoulder-and-elbow/3053/slap-lesion
If there are any symptoms with a superior labral tear, they are likely to include pain or clicking with activity, and decreased speed (velocity) and accuracy with throwing or hitting. Multiple studies, including some with our USA Volleyball National Team athletes, show that labral tears are quite common in post high school athletes and that in many cases they do not lead to any symptoms or decrease in performance.
The presence of symptoms or a decrease in performance dictates the course and goals of treatment for superior labral tears, not just finding the presence of a superior labral tear on advanced imaging (such as MRI).
Reviews of shoulder mechanics have identified certain abnormalities that increase the chance of superior labral tears in overhead athletes. Just as there are 3 different joints that make up the shoulder complex, there are 3 common mechanical issues that increase the risk for superior shoulder labral tears.
- Tightness in the front of the shoulder where the pectoralis minor and short head biceps brachii tendons attach to the coracoid that comes off the scapula bone. This can rotate the position of the glenoid and cause abnormal contact forces at the superior labrum.
- A scapula that is lower, pulled outward, rotated downward and comes off the chest wall can also lead to abnormal contact forces at the superior labrum.
- Tightness of the capsule and muscles behind the glenohumeral joint will limit internal rotation (follow-through) and increase shear forces at the biceps tendon/labrum connection
From school-age through collegiate athletes to professional and Olympic-level athletes with overload labral tears that cause symptoms or affect performance, starting with non-surgical therapy that address these 3 common mechanical issues is often preferable to surgical repair.
Surgical repair recreates good looking labrum anatomy often at the cost of loss of motion leading to reduced power, velocity and accuracy (especially in baseball pitchers). Typically, repetitive overload shoulder labral tears don’t require surgical reconstruction as a first-line option. It is usually a down-the-road option only after failure of a diligent and consistent therapy program to reduce symptoms of repetitive overload shoulder labral tears.
RELATED CONTENT: PREVENTING SHOULDER PAIN
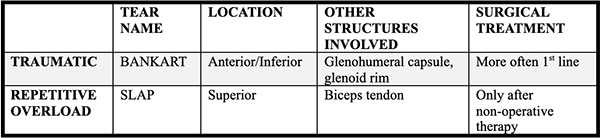
In summary, here are the two most common types of shoulder labral tears:
